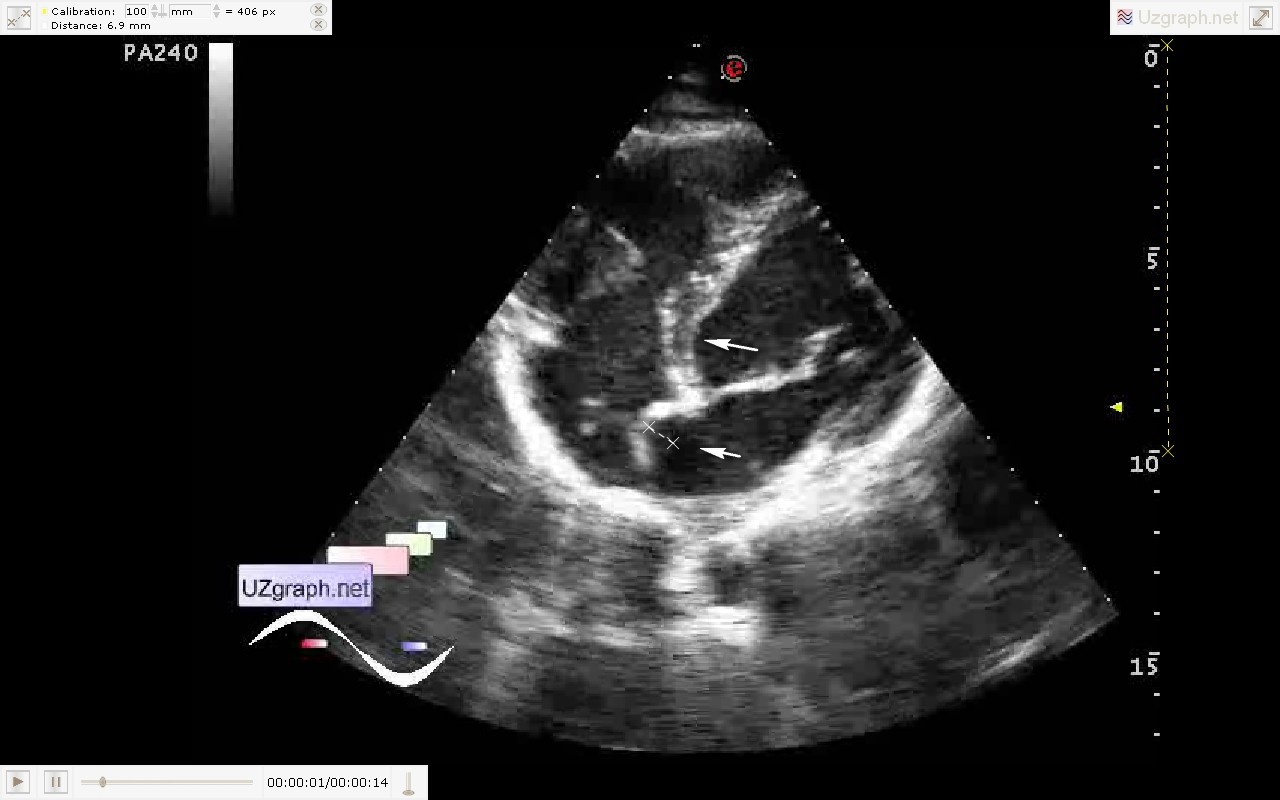
Progressive sonologists which do the echocardiography thinking with scepticism about such diagnoses as patent foramen ovale(PFO), mitral valve prolapse(MVP), false chord LV, by analogy with the sand in the kidney. So I thought about another such diagnosis - atrial septum aneurysm(ASA). What is the importance of an isolated ASA in medical practice? Any bending of AS should be considered as an aneurysm? Case for an example, Teen 14 years old came to echocardiography, long was seen with an ASA, due to which he is not allowed to play sports. Also cardiologist record that previously on echocardiography was detected elongated eustachian valve. At US in RA is rendered floating linear structure emanating from the region of IVC (eustachian valve?) In oblique projection of the 4 chamber view really seen bending of AS to RA up to 6 mm from the base line of AS, but there is not in the standard projection. In the same oblique projection, in which is seen bending AS, also can be clearly seen the bending of IVS. So I jokingly said to accompanying the child parent that if colleagues here believe that there is an ASA, then there is an aneurysm of IVS too.  Or, as one friend of mine said - I can make the US-picture of such pathology, which isn' t really present! Or, as one friend of mine said - I can make the US-picture of such pathology, which isn' t really present! All of this is qualitative assessment, which in most cases we use, and how to be with quantitative assessment? All bends of AS is really ASA? Here, for example, a quote from the Medscape: " Atrial Septal Aneurysm Diagnostic criteria for ASA established by Hanley based on the appearance on echocardiography are: aneurysmal dilatation of the atrial septum protruding at least 1.5 cm beyond the plane of the atrial septum or phasic excursion of the interatrial septum during the cardiac cycle of at least 1.5 cm in total amplitude with a diameter at the base of the aneurysm of at least 1.5 cm.[2] The condition can also be described using the Olivares-Reyes criteria, a classification based on the extent of excursion into each atrium.[3] Atrial septal aneurysm is clinically significant because of its association with cryptogenic stroke especially when there is a concurrent PFO. Approximately 70% of patients with ASA also have a PFO, while PFO is present in only 22% of patients without ASA. In one study, the combination of ASA and PFO was associated with a 33-fold higher risk of cryptogenic stroke.[1] 1 Cabanes L, Mas JL, Cohen A, et al. Atrial septal aneurysm and patent foramen ovale as risk factors for cryptogenic stroke in patients less than 55 years of age. A study using transesophageal echocardiography. Stroke. 1993;24:1865-1873. 2 Hanley PC, Tajik AJ, Hynes JK, et al. Diagnosis and classification of atrial septal aneurysm by two-dimensional echocardiography: Report of 80 consecutive cases. J Am Coll Cardiol. 1985:6: 1370-1382. 3 Olivares-Reyes A, Chan S, Lazar EJ, et al. Atrial septal aneurysms: A new classification in two-hundred five adults. J Am Soc Echocardiogr. 1997;10: 644-656." external link Question - can it be the ASA without PFO? Yes. And what then is the significance of an isolated ASA without PFO? In fact, the same we can read about the PFO without ASA! I.e. speaking about the risk of paradoxical embolism from right to left, from the veins of the LE(lower extremity) to a system circle, you need a shunt! ASA is a shunt? No! Then have an ASA contraindication to sport ?! PFO is a contraindication to sport? No, this is the normal variant. For the development of paradoxical embolism for begining we need a DVT(deep vein thrombosis)! And, of course, with vein thrombosis of LE can not play sports, whether there is a PFO or not - pulmonary embolism (PE) - it is also extremely dangerous! And here already paradoxical embolism is secondary. I.e. comparing ASA with MVP without regurgitation, what is its significance? Zero! Well, if we replace, for example, it by the ball or disc prostheses? Their shape is normal? For us it does not matter - the shape of the valve - if it is working properly! Because our task is not to find a some mismatching of person parameters with a some standard of shape, i.e. not to create a problems for a person from scratch but to solve the real problems - bearing a threat to life! external link |