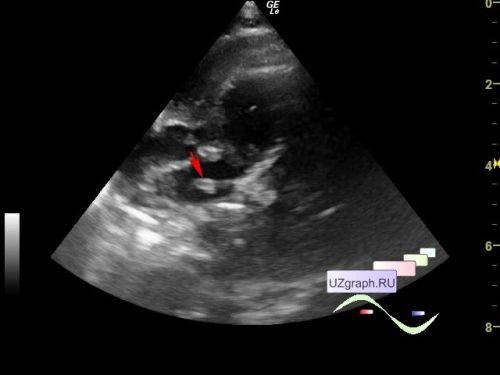
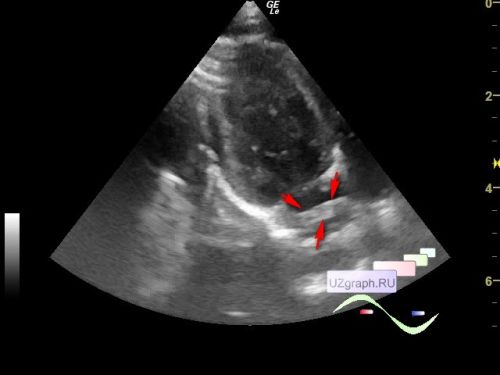
Child 1 month old at the planned screening ultrasound in the public clinic.
On echocardiography in the projection of the cavity of the left atrium / left atrial appendage, a linear hyperechoic structure up to 12x4 mm is visualized (differential diagnosis: incomplete septum, myxoma, etc.)
Echocardiography of the second opinion in the cardiology center was recommended.
Discussion:
"The left lateral “ridge” between the appendage and the left pulmonary veins was first described by Keith in 1907 as the “left tenia terminalis.” It is recognized as a Q-tip sign on echocardiographic imaging and, when prominent, can be mistaken for a thrombus or atrial mass. Integral to the ablation line for isolating left pulmonary veins, this “ridge” is actually an infolding of the lateral atrial wall. The fold is narrower at its superior border with the left superior pulmonary vein compared with its border with the inferior pulmonary vein (2.2–6.3 mm versus 6.2–12.3 mm). In 75% of the hearts studied, the fold is less than 5 mm wide and its profile of the fold varies from being flat, round, or pointed... The fold has thicker muscle in the anterosuperior portion. Within the fold runs the remnant of the vein of Marshall, abundant autonomic nerve bundles, and a small atrial artery which, in some cases, is the sinus nodal artery... A study on postmortem hearts revealed that the Marshall remnant is less than 3 mm from the endocardial surface and that the fold has muscular connections to the pulmonary veins."
"Excluding the atrial appendage, the walls of the left atrium are fairly smooth on the endocardial aspect although of non-uniform thickness. Viewed from inside the atrium, the walls are perforated by orifices of the pulmonary veins, atrial appendage, and the mitral valve. Thus, in-between the ipsilateral pulmonary venous orifices are the interpulmonary ridges. There is usually a prominent ridge in between the os of the atrial appendage and the left superior pulmonary venous orifice... It is recognized as a Q-tip sign on echocardiographic imaging. When prominent, it can be mistaken for a thrombus or atrial mass. Termed the posterolateral ridge, this is an infolding of the left atrial wall. In cross-section across its narrowest part, the profile of the fold is rounded in 75% of heart specimens, flat in 15%, and pointed in 10% with implications for catheter stability when ablating along the ridge... The fatty tissues on the epicardial side of this fold contain atrial arteries, nerve bundles, as well as the oblique vein of Marshall or its remnant that descends to join the coronary sinus. This vein is obliterated for the most part, but it remains patent as the persistent left superior caval vein which occurs occasionally as an isolated malformation in the normal population."
"A coumadin ridge, also called warfarin ridge or left lateral ridge, is a band-like embryological remnant in the left atrium between the left superior pulmonary vein and the left atrial appendage. It is considered an anatomical variant.
The ridge is formed by the coalition of the left superior pulmonary vein and left atrial appendage, which results in a lateral fold of left atrial wall tissue. The ridge contains the ligament of Marshall, autonomic nerve bundle, and small atrial or sinoatrial node artery."
And everything seems to be clear, here it is the answer - the left lateral ridge, which is sometimes confused with blood clots and lesions (everything is simple), but a small fly in the ointment for lovers of simplicity ...
"An atypical case of left atrial myxoma
...
Transthoracic echocardiography revealed a large (22 mm x 26 mm) mobile left atrial (LA) mass attached to the lateral wall... Transesophageal echocardiography showed a highly mobile heterogeneous oval pedunculated mass attached to the coumadin ridge and protruding into the LA appendage (LAA) during atrial systole."
In other words, it can not only imitate a myxoma, but a myxoma can actually grow from it, i.e. there is evidence that this ridge can be confused with lesions, what a pity that there is no evidence to the contrary, i.e. how many small mixomas and clots were missed due to mistaking them for this ridge?