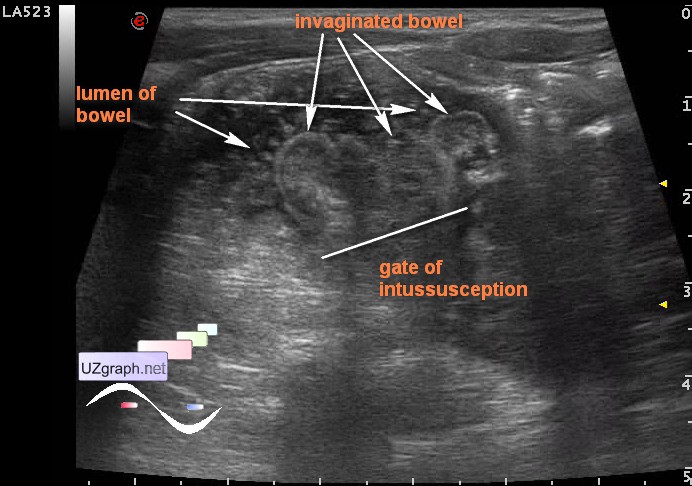
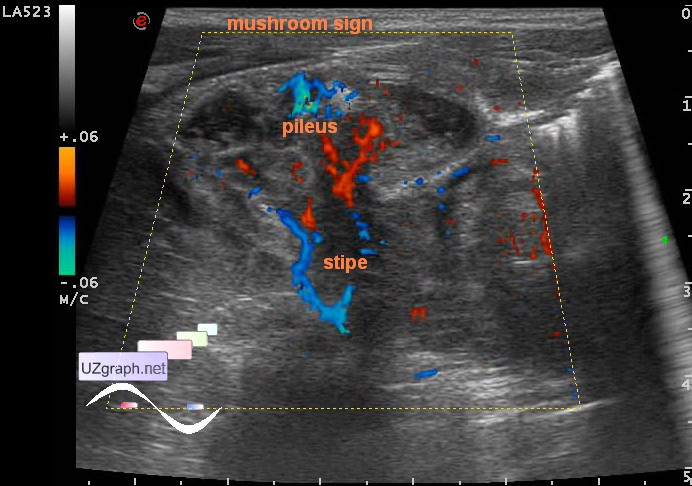
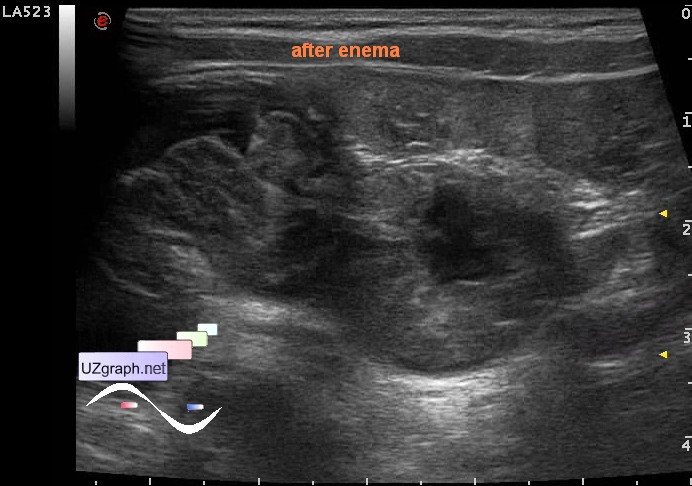
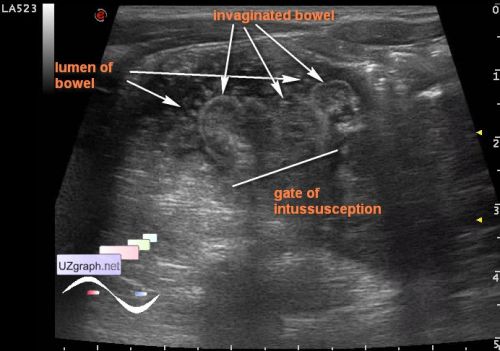
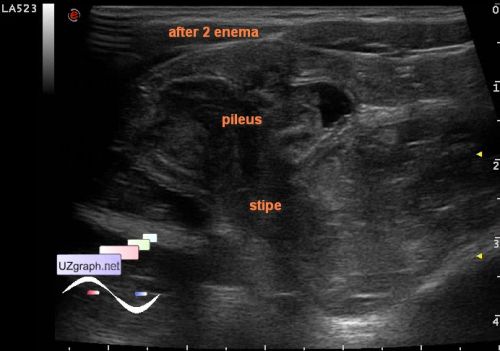
Child 2 years old with suspected appendicitis or intussusception. At US in the lower right quadrant of the abdomen visualized version of the target sign at CFM with bloodstream (dif.diagnosis: ileocecal intussusception, ileotyphlitis, etc.). In most parts of the abdomen expanded bowel loops with heteroechoic content. The essence of this version of the target sign, atypical target: central target element - spastic colon invaginated into the wall of the expanded intestine with fluid, in longitudinal section there is a mushroom sign. Two straightening attempts have been made through an enema, at ultrasonography without essential dynamics. After the first enema at the base of "mushroom" appeared bowel segment with a thickened wall to 9mm. PS. Difficulties in differentiating ileotyphlitis and ileocecal intussusception include the fact that, in my experience, intussusceptions lead to a thickening of the wall of the intestinal segment that was in the intussusception by the type of hematoma, so after straightening the intussusception, the echo-pattern of the intestinal area that was in the intussusception may correspond to that in enterocolitis, moreover, these processes can be present simultaneously. "The main complications of ileal TB are: Massive hematochezia (that can be controlled by endoscopic coagulation therapy), bowel obstruction (14%-32% of the cases), necrosis and intestinal perforation (1%-15%), enterocutaneous fistula (2%), ileoileal fistula, mesenteric lymphadenitis with intussusception, ileal loops or intestinal volvulus (2%), ascites, purulent or stercoral peritonitis (1%-10%), septicemia, psoas abscess, liver abscess, portal hypertension in children, etc." external link external link |